
Psilocybin Rules: My Comments to the Oregon Health Authority
The agency should strengthen rules on client confidentiality, product labeling, microdosing, client support persons, intoxicants, license fees, community use, consumption limits, and video recording


For nearly two years, the Oregon Health Authority (OHA) has drafted rules for implementing Measure 109, the Oregon Psilocybin Services Act. Passed by voters on November 3, 2020, this ballot initiative legalized the supported adult use of psilocybin, a psychedelic compound produced by many species of fungi. But before psilocybin businesses open in 2023, Measure 109 requires the OHA to publish final rules for the industry by December 31, 2022.
The agency adopted a first set of rules in May, which covers psilocybin manufacturing, facilitator training, and product testing. Remaining issues are addressed in a second set of rules. The OHA published a first draft of these rules in September, followed by a revised draft in November. This second set of rules addresses client confidentiality, psilocybin administration, facilitator responsibilities, product labeling, and other assorted topics.
From November 1st to 21st, the OHA received written public comments on the latest draft rules. It hosted live comment sessions from November 15th through 17th. Public comments are now closed while the agency finalizes its rules by year’s end.
Below I provide the remarks I submitted to the OHA during the November comment period. I urge the agency to improve its rules regarding client confidentiality, product labeling, microdosing, client support persons, intoxicants, license fees, community use, consumption limits, and video recording.
Client confidentiality is one of the most important issues facing the OHA, and my detailed thoughts on the topic can be found in Seeking Psychedelics? Check the Data Privacy Clause and Oregon Psilocybin Emails Show Secret Data Collection Plans. Becasue the confidentiality issues are fairly complex, my recommendations to the OHA are somewhat technical. One must analyze the text of Measure 109 to understand how it stronly protects client confidentiality while the OHA’s current rules do not.
If you have thoughts on my suggestions, please post them below the article. The following comments have been lightly edited to suit this online format.
I thank the Oregon Health Authority (OHA) for drafting many sensible rules for implementing Measure 109, the Oregon Psilocybin Services Act. Examples include the prohibition on exercising the privileges of other professional licenses while providing psilocybin services, separating service centers from licensed healthcare facilities, allowing for lower dose administration sessions of correspondingly shortened duration, and allowing group sessions that will help reduce costs.
However, many draft rules pose unnecessary risks to clients or make Oregon’s psilocybin services inaccessible to aspiring clients, facilitators, and business owners.
Please consider amending the rules as follows:
Clarify that clients are not required to share deidentified data with anyone outside service centers for research or other purposes unless they unambiguously opt-in, and specify that clients are not required to opt-in as a condition of receiving psilocybin services
As approved by voters, the Oregon Psilocybin Services Act (Measure 109) contains robust client confidentiality protections. These safeguards were codified in the Oregon Revised Statutes (ORS) under Section 475.450.
ORS 475A.450, titled “Confidentiality of client communications, information; exceptions,” states “[a] psilocybin service center operator, a psilocybin service facilitator, or any employee of a psilocybin service center operator or psilocybin service facilitator may not disclose any information that may be used to identify a client, or any communication made by a client during the course of providing psilocybin services or selling psilocybin products to the client.”
ORS 475.450 has two parts. The first addresses the disclosure of information that may be used to identify clients. The second part addresses the disclosure of any communication made by clients during the course of providing psilocybin services or selling psilocybin products. The term “any communication” is extremely broad. It clearly includes written, verbal, and nonverbal forms of communication, including gestures and other behaviors, that convey information. It may also include physiologic measurements taken from clients, such as heart rate and other biometric data, that communicate information to facilitators.
Moreover, like the first part of ORS 475.450, the second part applies to all stages of psilocybin services, including preparation, administration, and integration sessions. The meaning of this second part is clear. Service center operators, facilitators, and employees cannot disclose any communications made by clients unless one of a several stated exceptions is met, most of which will be rare. However, Item Number 16 of the Informed Consent Document (Rule 333-333-5040) misrepresents ORS 475.450 and the rights it creates to safeguard clients.
a. Item Number 16 of the Informed Consent Document (333-333-5040) fails to acknowledge that the same exceptions that apply to the first part of ORS 475.450 also apply to the second part of ORS 475.450
Both parts of ORS 475.450 must be given legal effect. However, the OHA’s current draft rules, and previous versions of those rules, appear to overlook the second part of ORS 475.450. For instance, in item number 16 of the Informed Consent Document (333-333-5040), OHA informs clients of only the first part of ORS 475.450 and the exceptions that apply, while omitting any mention of the second part of ORS 475.450, regarding any communications made by clients, and the fact that the same exceptions apply. Consequently, Item Number 16 of the Informed Consent Document fails to adequately inform clients regarding the conditions in which service center operators, facilitators, and employees can disclose their communications.
Please amend Item Number 16 of the Informed Consent Document by including the second part of ORS 475.450, which addresses “any client communications,” and make it clear to clients that the same exceptions that apply to the first part of ORS 475.450 apply to the second part.
b. Delete Item Number 15 from the Informed Consent Document (333-333-5040)
Item Number 15 of the Information Consent Document (333-333-5040) misinforms clients by leaving the impression that the exceptions that apply to ORS 475.450 do not apply to deidentified data. Item Number 15 also requires clients to agree to share their de-identified information with third parties outside service centers “for research or other purposes,” as a condition of receiving psilocybin services in Oregon. However, de-identified data would fall within the catchall term “any communication made by clients,” in the second part of ORS 475.450, which does not differentiate between communications that contain personal identifiers, communications that never contained personal identifiers, or communications from which personal identifiers have been removed. The second part of ORS 475.450 simply refers to “all communications.”
This interpretation is supported by the fact that the first part of ORS 475.450 arguably refers to information that has been de-identified. If the second part of ORS 475.450 only applied to information that could be used to identify clients, then it would be redundant because the first part of ORS 475.450 already addresses that kind of information. Moreover, communications made by clients need not contain personal identifiers. For instance, the statements “I am tired” and “the room is warm” contain no personally identifiable information. Yet because they are communications made by clients, they would be protected by the second part of ORS 475.450. Consequently, they could not be disclosed unless one of the enumerated exceptions applies. Taken together, the first and second parts of ORS 475.450 indicate that it does not matter whether client information has been de-identified, no client information can be disclosed unless one of the exceptions lister under ORS 475.450 is met.
Item Number 15 in the Informed Consent Document could be perceived as an attempted work around to circumvent the second part of ORS 475.450. By requiring clients to agree to share de-identified data, it removes any meaningful ability of clients to choose and attempts to manufacture one of the exceptions, namely client consent. The only reasonable interpretation of ORS 475.450 is that Measure 109 intended to give clients who are participating in Oregon’s psilocybin services an actual choice whether to share deidentified or personally identifiable data, which does not impact their ability to receive services.
During the latest three public comment sessions, the OHA heard from numerous commentators who are deeply concerned that the draft rules require clients to agree to share de-identified data with third parties outside of service centers. One commentor referenced the history of immoral unauthorized experimentation on marginalized communities. Another referenced the potential for commercial exploitation of clients’ deidentified data.
Forced sharing of their deidentified data exposes clients to social, professional, and legal risks because psilocybin remains a stigmatized substance that is federally illegal. If people’s participation in Oregon’s psilocybin services is revealed to third parties, clients could lose their jobs, their homes, and a variety of benefits.
Many experts believe that there is no such thing as anonymized or de-identified data. Please see the following article by Professor Paul Ohm, titled Broken Promises of Privacy: Responding to the Surprising Failure of Anonymization, to understand the risks associated with deidentified or “anonymized” data.
I also refer you to my recent article in Wired, titled Seeking Psychedelics? Check the Data Privacy Clause. In this article, several experts without interests in the psilocybin industry express serious concerns with OHA’s current draft rules and the requirement that clients agree to share deidentified data.
Please respect the voters will and leave the choice regarding whether to share data with the clients that ORS 475.450 was drafted to protect.
In emails sent between OHA’s Angela Albee and representatives of the Healing Advocacy Fund, Albee makes clear that OHA cannot require psilocybin facilitators to share client information, including deidentified data, outside service centers. Forcing clients to agree to share deidentified data outside service centers is no better. It breaches the public’s trust and violates the meaning of consent.
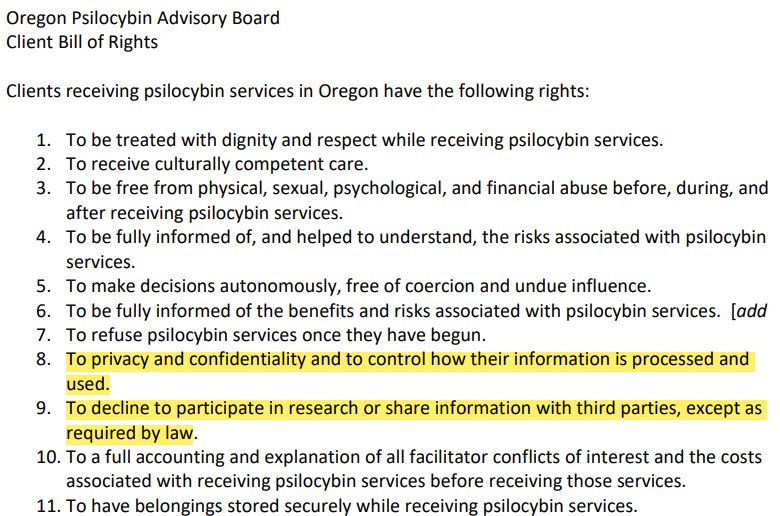
c. Implement the Oregon Psilocybin Advisory Board’s past recommendations for the Client Bill of Rights (333-333-4520) regarding client control of information and participation in research
In May, the Oregon Psilocybin Advisory Board unanimously approved giving clients the right to control how their data is processed and used and to decline to participate in research or share information with third parties. These recommendations were omitted from OHA’s draft rules. Please include the Board’s recommended language for the Client Bill of Rights (333-333-4520) as highlighted in yellow below.
d. Implement the Oregon Psilocybin Advisory Board’s past recommendations regarding a duty of confidentiality for facilitators
In May, the Oregon Psilocybin Advisory Board recommended duties for psilocybin facilitators, including a duty of confidentiality that required facilitators to “attempt to maintain the confidentiality of client information to the greatest extent possible.” This and other recommended duties were omitted from OHA’s draft rules. Please introduce the Board’s duty of confidentiality into the OHA’s final rules as highlighted in yellow below.

e. Please include the Oregon Psilocybin Advisory Board’s approved Statement on Data Collection at the top of the Informed Consent Document (333-333-5040)
In June, the Oregon Psilocybin Advisory Board unanimously approved a Statement on Data Collection, which warned clients of the risks of sharing their data with third parties outside service centers, including the potential for deidentified data to reveal their identities and their participation in Oregon’s services. This Statement on Data Collection was not included in the Informed Consent Document (333-333-5040) in OHA’s current draft rules. Please introduce the Statement on Data Collection approved by the Board into OHA’s final rules at the top of the Informed Consent Document as recommended by the Board earlier this year.
Update labeling requirements in (333-333-2400) to require the inclusion of solvents, pesticides, and allergens
Please include solvents, pesticides, and common allergens in the section on labeling for sale to client (333-333-2400). Clients deserve to know what substances they may be exposed to when consuming psilocybin products, including the solvents used to extract psilocybin, the pesticides applied during the cultivation of psilocybin producing fungi, and common allergens that may pose a risk of anaphylaxis to people with food allergies.
Including potential allergens on product labeling is crucial to promoting client safety because having an allergic reaction while under the influence of psilocybin could be unecessarily frightening, life-threatening, or fatal. These incidents are easily prevented by requiring the inclusion of common allergens on psilocybin product labels.
In the section on duration of administration sessions (333-333-5250), please create a lower tier for doses of 2.5 milligrams or fewer with no minimum duration requirement
In 333-333-5250, please create a lower tier for doses of 2.5 milligrams of psilocybin or fewer with no minimum duration. There is growing interest in the practice of microdosing, and people who wish to microdose should have the opportunity to benefit from Oregon’s regulated psilocybin program. Measure 109 allows for microdosing and mandates no minimum duration for administration sessions.
When clients consume low doses of psilocybin, which are subperceptual, it would be unduly burdensome and expensive to require people to remain at service centers for a minimum of one hour. For people who have not consumed psilocybin previously, it may be sensible to implement a one-hour minimum duration for their first administration session. However, beyond that, mandating a minimum is likely to encourage people to avoid the regulated system and turn to the unregulated market.
Creating opportunities for microdosing within the regulated system is a harm reduction measure because it encourages people to consume psilocybin products that were manufactured under controlled conditions and administered by trained facilitators.
Increase the ability of clients to bring loves ones and other supportive individuals to administration sessions by amending the section on Interpreters and Client Support Persons (333-333-5070)
Please make it easier for clients in the psilocybin program to bring other people into their administration sessions, which can increase comfort and safety.
Consuming psilocybin can be a stressful experience for some clients. Having a friend or love one present may reduce anxiety and increase the likelihood of having positive psilocybin experiences. This change could be achieved by expanding the definition of client support person to include anyone clients designate for this role.
Amend the current prohibition against intoxicant use by facilitators under the section on Prohibited Conduct (333-333-6000)
The current definition of intoxicant in the section on Prohibited Conduct (333-333-6000) is too broad, and the rules regarding intoxicant use by facilitators are overly restrictive. They may discriminate against facilitators who safely use legally obtained or prescribed intoxicating substances that would not interfere with their capacity to competently perform their duties.
I suggest amending this rule to constrain the definition of intoxicants and allow facilitators to use legally obtained intoxicating substances that when used correctly are unlikely to interfere with their ability to competently perform their duties.
Reduce license fees (333-333-4060) for facilitators and nonprofit organizations
The Oregon Health Authority has heard from many commentators that the annual fees for licensed psilocybin businesses and practitioners are too high. In the interest of reducing barriers to entry and encouraging a diverse workforce in this emerging industry, please reduce the license fees for facilitators and non-profit organizations, even if it means raising fees for other licensed businesses.
Create rules that are tailored to religious and spiritual communities
Even though Measure 109 created a non-medical access model for psilocybin, many of the people involved in implementing Measure 109 view psilocybin only from a healthcare perspective. Other perspectives, such as those of religious, spiritual, and Indigenous communities have often been overlooked or marginalized in the rulemaking process. Accordingly, I ask that you create rules that make Oregon’s emerging psilocybin industry more accessible for spiritual, religious, and Indigenous communities.
The OHA rejected the entheogenic framework proposed by Jon Dennis because the Oregon Department of Justice (DOJ) and OHA felt the framework would privilege religious practice and pose an establishment clause problem. However, the rules governing Oregon’s psilocybin services are currently unwelcoming to spiritual, religious, and Indiginous communities, while arguably privileging healthcare providers.
The proposed entheogenic framework would not have given religious or spiritual communities an advantage in the industry. Instead, it merely would have helped to put them on equal footing with healthcare providers. Moreover, because the entheogenic framework applied equally to religious and spiritual communities, it did not specifically promote religious practice nor pose the establishment clause issues identified in the DOJ memo to OHA.
In the interest of harm reduction, please eliminate the 50 milligram dose limit in the section on Consumption Limits (333-333-5240)
Regardless of the rules that OHA implements, some people will want to consume more than 50 milligrams of psilocybin. Establishing a dose limit merely encourages people to consume higher doses outside the regulated framework without professional supervision. It would be preferable to eliminate the dose limit and provide a warning to clients that although consuming more than 50 milligrams of psilocybin in a single administration session is allowed, it is not encouraged. Please eliminate the 50 milligram dose limit in the rule on Consumption Limits (333-333-5240).
Video Recordings of Administration Sessions (333-333-4640)
To protect client confidentiality, the Oregon Psilocybin Advisory recommended that surveillance cameras not be allowed in client administration areas. An earlier version of the OHA’s draft rules allowed facilitators to video record administration sessions using portable equipment with client consent, and clients could request to have the recordings deleted. However, the current draft rules require service centers to maintain video recordings for 5 years and clients cannot request their deletion.
To protect client confidentiality, please return the client right to request deletion to OHA’s rules. In addition, please require video recordings to be deleted automatically after 30 or 60 days unless a report of abuse or other violation of administrative rules is reported to OHA.
The current draft rules appear to provide OHA unrestricted access to video recordings of client administration sessions. Please amend those rules to allow OHA access to video recordings only if one of the exceptions to client confidentiality stated in ORS 475.450 applies.
Respectfully,
Mason Marks, MD, JD
*The views expressed on Psychedelic Week do not represent the views of POPLAR at the Petrie-Flom Center at Harvard Law School or the Florida State University College of Law. Psychedelic Week is an independent project unaffiliated with these programs and institutions.
Mason Marks, MD, JD is the Florida Bar Health Law Section Professor at the Florida State University College of Law. He is the senior fellow and project lead of the Project on Psychedelics Law and Regulation (POPLAR) at the Petrie-Flom Center at Harvard Law School and an affiliated fellow at the Information Society Project at Yale Law School. Marks teaches constitutional law, administrative law, drug law, and psychedelic law, . Before moving to Florida, he served on the Oregon Psilocybin Advisory Board where he chaired its Licensing Subcommittee. Marks has drafted drug policies for state and local lawmakers. His forthcoming book on psychedelic law and politics will be published by Yale University Press. He tweets at @MasonMarksMD and @PsychedelicWeek.